
A Portfolio Lens for Introducing Health Innovations
Figuring out the right questions to ask when introducing new health innovations: building on South Africa's portfolio approach




Here’s the puzzle: How can an innovation be clinically sound, financially approved, and still operationally fragile?
Part of the answer lies in how health products are prioritised and introduced within the health system. Too often, products are assessed one at a time, through processes that may not fully consider system readiness, implementation requirements, or how each product contributes to broader national health priorities. Health leaders first need to ask whether a new device, diagnostic, medicine, or vaccine is needed, safe, effective, and affordable. But those product-level questions are not enough. Whether it can be introduced effectively also depends on its fit with national priorities, budgets, programmes, care pathways, delivery platforms, procurement systems, and workforce capacity.
That is why a portfolio-based approach matters. As part of the ALIGN framework, such an approach does not replace product appraisal. It strengthens the next layer of decision-making – how well the product fits national priorities, system capacity, available resources, and the wider product pipeline.
To inform this work, ALIGN-South Africa reviewed 20 health products introduced into South African policy. The review highlights where portfolio logic is already present and where it could be applied more systematically.
A good product is not enough
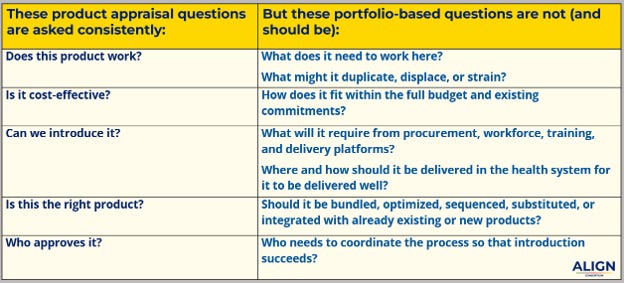
Health leaders typically begin with a set of essential product-level questions: Is this device, diagnostic, medicine, or vaccine needed? Is it safe and effective? Will people use it? Is it cost-effective and affordable?
These questions are necessary for prioritising and introducing health products. They help establish whether an innovation has value on its own terms.
But this familiar product-by-product appraisal is insufficient. Without a clear view of system fit, it can create a false sense of feasibility and value. A product may have strong clinical evidence and good individual cost-effectiveness marks, yet still strain the overall budget, workforce, procurement system, or delivery platform needed to introduce it well. Here’s why:
New health products do not enter an empty space. They enter and must integrate within existing—but often strained—treatment programmes, budgets, procurement systems, workforce capacity, and delivery platforms (e.g., Australia’s REACH trial).
New health products do not arrive one by one. Multiple products may be introduced to the system simultaneously or in close succession, competing for the same budget, workforce, training systems, supply chains, and policy attention. How products are prioritised and sequenced can therefore shape whether they collectively advance health needs and national goals (e.g., Uganda’s use of SMART Vaccines 2.0).
This is where a portfolio-based approach adds value. It does not replace one-off product evidence-informed appraisal; it complements decision-making by adding a system and portfolio lens. By more explicitly considering system fit, sequencing, and interdependencies, portfolio-based planning helps decision-makers assess not only whether a product works, but also whether it can be introduced well alongside other priorities.
South Africa already uses portfolio logic in some policy areas
In South Africa, a portfolio-based approach is not an outside concept or a new layer of bureaucracy. Such an approach is already evident in the way health products are considered alongside existing treatment options, care pathways, delivery platforms, and programme priorities. Several policy areas show portfolio logic, including:
Integrated HIV/TB/STI service delivery
The challenge is that this logic often remains implicit—shaped by programme experience, budgets, procurement systems, workforce capacity, and delivery structures—rather than being clearly named and systematically applied.
Across our review of 20 health products and 166 decision points in South Africa, three findings stand out:
1. Strong foundations exist for evidence appraisal and coordination
South Africa already has robust mechanisms for evaluating individual products: across all 20 cases, we found that technical review processes and institutional oversight were consistently present—an important strength to build on. A portfolio-based approach does not replace these mechanisms. It complements them by asking how products fit together and how they can be introduced in ways that strengthen―rather than strain―the existing health system.
2. Portfolio-based approaches are present—but often remain implicit
In several cases, products were considered in relation to existing products, platforms, or care pathways. But these decisions were rarely framed as “portfolio-based” or used as a standard comparative decision step.
The clearest examples show up in five familiar forms in South Africa:
Bundling products or interventions within a care pathway
Optimising the treatment mix by assessing how a product fits within existing treatment options
Substitution within an existing treatment mix
Sequencing products over time
Platform integration through established delivery systems
A few examples from our research highlight these forms:
Example 1: South Africa’s HIV programme illustrates treatment-mix optimisation and substitution. The introduction of dolutegravir (DTG) was not simply the addition of a new medicine; it reshaped treatment across adult care, maternal health, and prevention of mother-to-child transmission. This strengthened coherence across the broader ART platform.
In contrast, the introduction of tenofovir alafenamide (TAF) reflected selective substitution. Rather than replacing standard regimens, it expanded treatment options for specific patient groups unable to tolerate existing therapies, including HIV care and chronic hepatitis B.
In both cases, the policy question was not simply whether to introduce the new product, but where it should sit within existing treatment options, care pathways, and programme priorities.
Example 2: Maternal health showing bundling within a care pathway. The introduction of tranexamic acid (TXA) for postpartum haemorrhage depended not only on the medicine itself, but also on its integration into a broader first-line care pathway. It included the WHO-endorsed E-MOTIVE bundle and South Africa’s standardised approach to postpartum haemorrhage care. Implementation required protocols, workforce training, referral pathways, supply chain readiness, and coordination with routine maternity services. The policy question was not simply whether TXA works, but how it should be delivered as part of a wider package of care.
Example 3: Prevention and public health illustrates platform integration and method-mix optimisation. South Africa’s human papillomavirus (HPV) vaccination programme used an established delivery platform―the Integrated School Health Programme―to reach adolescent girls at scale, showing how an existing delivery platform can support product introduction.
A similar logic applies to contraceptive products, including implants and self-injectables. For contraceptive products, the question is not simply whether to add another method. It is how each option expands choice, fits within the existing method mix, and can be delivered through platforms that are accessible, effective, and equitable. In these cases, the central policy question is not only whether to introduce a product, but also where and how it can be delivered most effectively and equitably.
Example 4: South Africa’s PCV pathway exhibits sequencing over time and adaptive substitution. South Africa’s pneumococcal conjugate vaccine (PCV) experience was not a one-off vaccine introduction. It evolved from PCV7 to PCV13 to address residual disease and expand serotype coverage, and later from PCV13 to PCV10 within the established Expanded Programme on Immunisation. This later switch was driven by procurement, affordability, and supply sustainability considerations, while retaining the same schedule and target population.
These examples point to a common lesson: health innovations are more likely to be introduced effectively when they are planned around shared care pathways, delivery platforms, and programme goals, rather than treated as standalone products or siloed programme decisions.
3. Visibility is highest in mature programme areas
Portfolio-based approaches appear most clearly in well-established programmes, including HIV, TB, immunisation, maternal and neonatal health, and laboratory diagnostics. This may be because mature programmes tend to have clearer guidelines, stronger delivery platforms, deeper implementation experience, and more established coordination processes.
The implication is important: where programmes are newer or more fragmented, portfolio questions may need to be made more explicit ―especially when new products are arriving quickly, budgets are tight, and delivery systems are already stretched.
The next step is moving from implicit practice to explicit policy
Taken together, the South Africa examples point to a practical lesson: portfolio-based planning does not need to be invented from scratch. The logic is already present in parts of the health system. The opportunity is to make it more visible, systematic, and useful for decision-making. This includes learning from integrated service delivery, care bundles, and vaccine portfolio management to ask better questions earlier— before major commitments are made on financing, procurement, training, and rollout.
Conclusion
South Africa’s experience shows that portfolio-based planning does not need to be invented from scratch. The logic is already appearing in how products are considered alongside treatment mixes, care pathways, delivery platforms, and system constraints.
The opportunity now is to make that logic explicit, intentional, and consistent, supported by better market data for decision-making, stronger government coordination, and more meaningful market engagement.
The goal is not simply to introduce more products. It is to introduce the right products, in the right combinations, at the right time, in ways that strengthen health systems rather than strain them—to ultimately benefit the people they serve.
 | A guest post by
|
 | A guest post by
|
 | A guest post by
|
 | A guest post by
|